prognosis of CML
Last edited 05/2019
Median survival is 4-6 years (can range from less than 1 year to more than 10 years)
- however occasionally patients die within a few months
- 3% of patients live more than 15 years without radical therapy
- once the accelerated phase is reached survival is usually less than 1 year and in the blast phase, few patients survive more than a few months (1).
It is important to identify the prognostic factors at diagnosis. The following can be used to provide useful prognostic information in a patient with CML:
- accurate identification of the disease stage (or phase) is considered to be the essential factor
- clinical and laboratory features - used to calculate prognostic scores (Sokal score or Hasford score)
- these scores identifies patients with low, intermediate, and high risk of short term survival
- cytogenetic changes e.g. - deletions of the derivative chromosome 9
- Imatinib can be used to partly overcome the negative prognostic effects of this
- but the size and location of the deletion appears to be important
- degree and timing of haematological, cytogenetic, and molecular responses (2)
Approximately 60% of young adults with successful allogeneic bone marrow transplantation are cured.
Studies have revealed that the following features are predictive of a shorter chronic phase:
- increased splenomegaly.
- older age
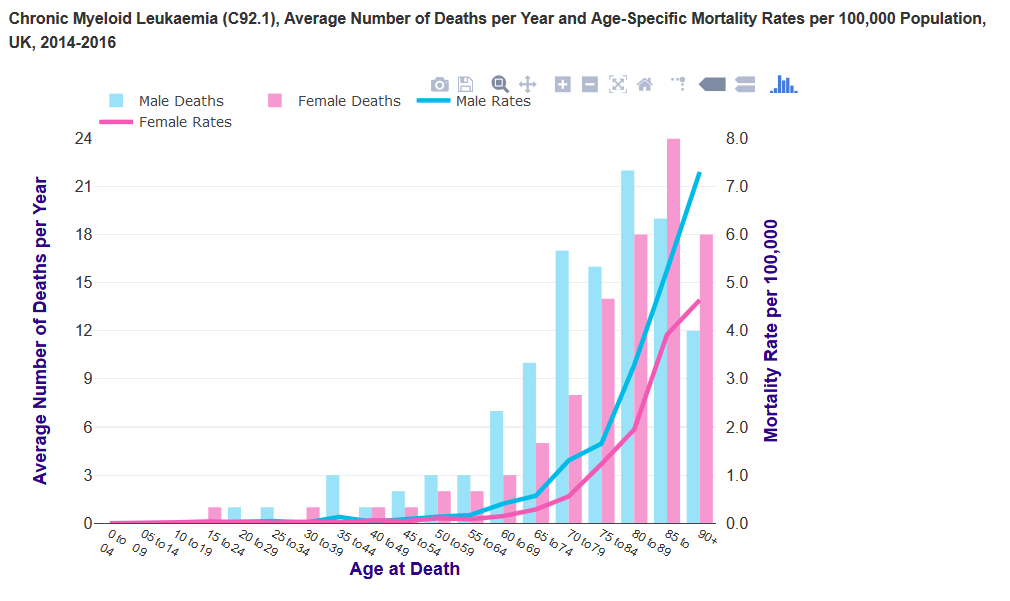
- chronic myeloid leukaemia mortality is strongly related to age, with
the highest mortality rates being in older people. In the UK in 2014-2016,
on average each year two-thirds (66%) of deaths were in people aged 75
and over
- largely reflects higher incidence and lower survival for chronic myeloid leukaemia in older people
- age-specific mortality rates rise steeply from around age 60-64. The highest rates are in the 90+ age group for males and females
- mortality rates are similar between males and females in most age groups
- chronic myeloid leukaemia mortality is strongly related to age, with
the highest mortality rates being in older people. In the UK in 2014-2016,
on average each year two-thirds (66%) of deaths were in people aged 75
and over
- male gender
- elevated serum lactate dehydrogenase.
- cytogenetic abnormalities in addition to the Ph1.
- a higher proportion of marrow or peripheral blood blasts.
- basophilia.
- eosinophilia.
- thrombocytosis.
- anaemia (1)
Reference: