assessment of clinical probability of pulmonary embolism (PE)
Last edited 05/2020 and last reviewed 01/2021
In patients with suspected PE, a clinical or pre-test probability assessment could be carried out based on the risk factors and clinical features
- it will assess the clinical likelihood of PE in a patient
- the assessment can be carried out either by implicit clinical judgement or by the use of a validated clinical prediction rule e.g.- Canadian rule, by Wells et al or the revised Geneva rule
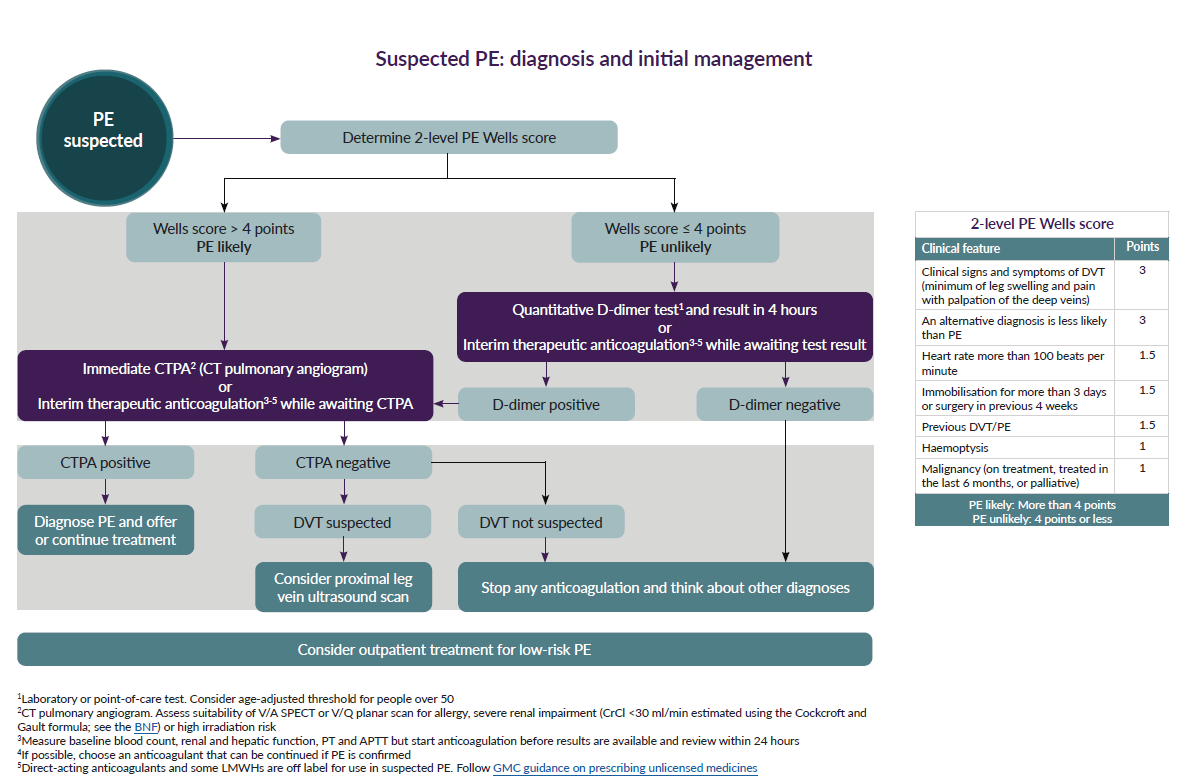
The Canadian rule by Wells et al divides a person's clinical probability of pulmonary embolism into:
- three-category scheme - low, moderate or high clinical probability
- two-category scheme - PE likely or PE unlikely (2)
The revised Geneva rule also divides the clinical probability of PE in to low, intermediate and high (2). Which ever rule is used the prevalence of PE is about:
- 10% - in patients with a low clinical probability
- 30% - in those with a moderate clinical probability
- 65% - in those with a high clinical probability
Concurrent use of a D-dimer test with the pre test clinical probability score is recommended. e.g. - when a negative d-dimer result is used together with a low or intermediate pre test clinical probability score, it has a 92% sensitivity at excluding pulmonary embolism (3)
A schemata for assessment has been suggested (4)
Reference:
- 1. Meyer G et al. Pulmonary embolism. BMJ. 2010;340:c1421
- 2. Torbicki A et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008;29(18):2276-315.
- 3. Robinson GV. Pulmonary embolism in hospital practice. BMJ. 2006;332(7534):156-60.
- 4.NICE (March 2020). Venous thromboembolic diseases: diagnosis, management and thrombophilia testing
Wells score in the clinical prediction of pulmonary embolus (PE)
Geneva rule in the clinical prediction of pulmonary embolus (PE)