thrombocytosis
Last edited 11/2019 and last reviewed 07/2023
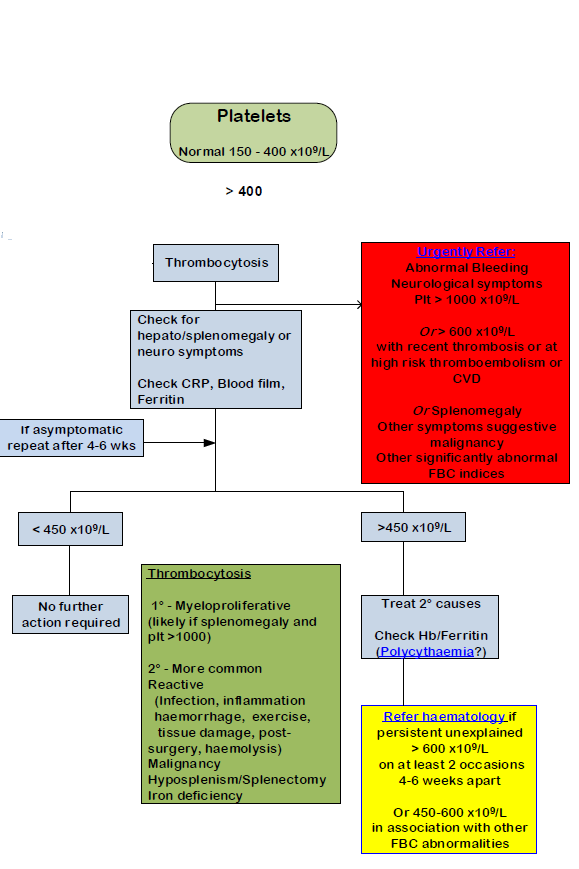
Thrombocytosis occurs when the platelet count exceeds 450 x 10^9/l although numbers may exceed 1,000 x 10^9/l without symptoms.
Thrombosis and paradoxically, haemorrhage are the main symptoms but their occurrence is as much dependent on qualitative defects in the platelets as much as their number.
Two types of thrombocytosis are recognised:
- reactive thrombocytosis - for which the term thrombocytosis properly reserved
- thrombocythaemia - an autonomous or essential thrombocytosis
A suggested management in adults (2):
Notes:
- in routine clinical practice, reactive thrombocytosis may be responsible
for more than 85% of cases with an increased platelet count
- causes of reactive thrombocythaemia (including inflammation, infection, haemorrhage and iron deficiency) must be excluded before a diagnosis of essential thrombocythaemia (ET)
- any degree of persistent thrombocytosis, whether or not it fulfils the conventional criterion of being above 600×109/l, must be pursued for the possible diagnosis of ET
- cases of unexplained thrombocytosis in adults may be due to cancer - consider further investigations such as a CXR, and OGD and faecal immunochemical test (FIT)
Reference:
- Elliott MA et al.Thrombocythaemia and pregnancy. Leuk Lymphoma. 1996 Sep;22 Suppl 1:57-63.
- NHS Camden CCG. Abnormal FBC guidance - for adults (Accessed 30/10/19)
essential thrombocythaemia (ET)
raised platelet count (thrombocytosis) - NICE urgent cancer referral guidance
thrombocytosis (raised platelet count) and subsequent cancer risk
faecal immunochemical tests (FIT) for hemoglobin and detection of bowel cancer